
Everyone knows sleep matters. The problem isn't awareness -- it's execution.
You've read the articles. You know you should sleep 8 hours. You know your HRV suffers when you don't. But at 3am when you're wide awake staring at the ceiling, or soaking through your sheets, or listening to a partner snore, generic sleep hygiene advice doesn't help much.
This article is different. It's organized by the actual reasons people can't sleep -- because the fix for stress-driven insomnia is not the same as the fix for night sweats, which is not the same as the fix for a racing mind before a big race. Finding what applies to you is the first step. Then the science gives you somewhere real to go.
What good sleep is actually doing for your training
Before the problems and solutions, a quick grounding in why this matters enough to take seriously.
Deep sleep triggers growth hormone release, which drives protein synthesis, stimulates amino acid uptake into muscle cells, promotes collagen synthesis for connective tissue repair, and supports bone mineral density. This is also when cortisol drops to its lowest levels -- creating a hormonal environment that is profoundly anabolic.
Even one night of sleep deprivation can reduce testosterone levels by nearly 25%, flipping the hormonal balance toward catabolism. This applies to both men and women -- testosterone is a recovery hormone for everyone, not just male athletes.
REM sleep handles the cognitive recovery side -- motor skill consolidation, reaction time, emotional regulation, and strategic decision-making all depend on it. Cut it short and you're slower, less coordinated, and less mentally resilient the next day regardless of how the rest of your training looks.
Research consistently shows that inadequate sleep impairs performance more than any other recoverable factor, while optimal sleep can enhance athletic performance by 10 to 15 percent. That's not a marginal gain. That's the difference between a good training block and a great one.
The sleep stages and why each one matters
Your device doesn't just track total sleep time. It tracks sleep architecture -- the sequence and proportion of stages you move through each night.
Light sleep (N1 and N2): The entry point and transition layer between deeper stages. N2 specifically plays a role in memory consolidation. Too much light sleep relative to deep and REM suggests fragmented sleep, even if your total hours look acceptable.
Deep sleep (N3 -- slow-wave sleep): The physiological engine of recovery. Growth hormone is released almost exclusively here. Cortisol is suppressed. Your body is in full repair mode. Deep sleep is front-loaded in the night -- going to bed very late costs you more deep sleep than almost any other habit.
REM sleep: Where your brain recovers. Motor learning, emotional processing, and reaction time are all consolidated here. REM is back-loaded -- it concentrates in the final hours of the night. This is why cutting sleep short from the end (early alarms, fragmented final hours) costs you disproportionate REM. A 7-hour night ending at 5am consistently strips more REM than the same 7 hours ending naturally at 7am.
The practical implication: Total sleep time matters. But so does timing. Going to bed consistently late compresses deep sleep. Waking consistently early compresses REM. Most athletes need 7 to 9 hours, with 8 to 10 hours during heavy training blocks, in a consistent window that protects both ends.
How sleep shows up in your training data
Poor sleep and compromised recovery produce nearly identical signatures in your wearable data. HRV drops. RHR rises. Readiness score falls. The data doesn't tell you why -- only that your body is under load. But when your training has been manageable and your readiness is still flagging, sleep is almost always the first place to look.
An increase in cortisol -- which sleep deprivation reliably drives -- yields a direct decrease in HRV. This is the physiological link between a poor night and a low readiness score the following morning. Conversely, consistently good sleep is one of the most reliable drivers of a rising HRV trend over time. Athletes who address their sleep first often see readiness data improve before they make any changes to training load.
Problem 1: You can't fall asleep or stay asleep (stress and racing mind)
This is the most common sleep complaint among athletes and working adults -- and it has a well-established, highly effective treatment that most people have never heard of.
What's happening
When you can't switch off, your sympathetic nervous system is still dominant. Cortisol is elevated. Your brain is running problem-solving loops it can't resolve. Sleep requires a parasympathetic shift your body hasn't made yet.
What the science says
Cognitive Behavioral Therapy for Insomnia (CBT-I) is considered first-line treatment for chronic insomnia by both the European Sleep Research Society and the American Academy of Sleep Medicine -- recommended before or instead of sleep medication. In plain terms, CBT-I is a structured program that changes the thoughts and behaviors keeping you awake -- not through medication, but through specific techniques that rebuild your body's natural ability to sleep. It combines sleep education with specific behavioral and cognitive techniques to restructure the thoughts and habits that perpetuate insomnia. It is not therapy in the traditional sense. It is a structured protocol that includes sleep restriction therapy, stimulus control, and cognitive restructuring -- and it has a higher long-term success rate than any sleep medication, with effects that persist after treatment ends.
What you can do tonight
- The 4-7-8 breathing technique: inhale for 4 counts, hold for 7, exhale for 8. The extended exhale directly activates the parasympathetic nervous system and has been shown to reduce sleep onset time
- Get out of bed if you've been awake for more than 20 minutes. Lying there frustrated reinforces the mental association between bed and wakefulness. Sit somewhere quiet with low stimulation and return when you feel genuinely sleepy -- this is a core CBT-I principle
- Write down tomorrow's worries before bed. A Baylor University study found that writing a to-do list of upcoming tasks before bed significantly reduced sleep onset time -- the act of offloading the list frees the brain from active processing
- Keep the room cool, dark, and phone-free. These aren't new but they remain the highest-return environmental adjustments
Problem 2: Night sweats and hot flushes (perimenopause and menopause)
This is one of the most disruptive and underaddressed sleep problems for female athletes in their 40s and beyond -- and it deserves a direct, honest answer rather than a footnote.
What's happening
Vasomotor symptoms including hot flashes and night sweats affect up to 80% of women during the menopause transition. They are caused by the hypothalamus -- the brain's temperature regulator -- becoming hypersensitive to small temperature fluctuations as estrogen declines. The result is an abrupt heat response that wakes you from sleep, often multiple times a night, fragmenting the deep and REM stages where recovery actually happens.
Research published in 2025 found that more severe evening hot flashes predicted longer sleep onset latency that night, and that more frequent nocturnal hot flashes were associated with worse sleep quality. The timing matters -- addressing the evening thermal environment is as important as the overnight one.
What the science says
Hormone therapy (HRT) is FDA-approved as the most effective first-line treatment for hot flashes and night sweats, with particular benefit when started in early menopause. For those who can't or choose not to use HRT, non-hormonal options with clinical support include CBT-I specifically adapted for menopause-related insomnia, and cognitive behavioral therapy for hot flashes (CBT-HF), which reduces the distress and perceived severity of flushes even when it doesn't reduce their frequency.
What you can do tonight
- Sleep in moisture-wicking technical fabric rather than cotton -- it moves sweat away from skin and reduces the cold-wet sensation that follows a flush
- Keep a small fan within reach for rapid temperature reduction when a flush starts, to minimize full waking
- Lower bedroom temperature to 16 to 18 degrees Celsius (60 to 65 Fahrenheit) -- a cooler baseline environment reduces the frequency and severity of nocturnal flushes
- Avoid alcohol entirely in the evening during symptomatic phases -- it's a vasodilator that reliably triggers flushes and fragments sleep architecture simultaneously
- Paced respiration during a hot flush -- slow deep breathing at 6 to 8 breaths per minute has been shown to reduce flush duration and intensity
- Track flush timing for one week alongside your Fit PA sleep data -- the pattern will help you and a healthcare provider identify the most targeted intervention
Problem 3: Snoring and suspected sleep apnea
This is the sleep problem most people joke about and least often treat -- despite it being one of the most significant performance limiters available.
What's happening
Snoring is the sound of partially obstructed airflow. Obstructive sleep apnea (OSA) is repeated full obstruction where breathing stops entirely for seconds at a time, triggering partial arousal each time the body forces itself to restart. Most people with OSA don't know they have it because they're unaware of the waking episodes. Their partner knows. Their HRV knows. They just assume they sleep poorly and leave it at that.
OSA is significantly underdiagnosed in athletes -- and particularly in women, whose symptoms often present differently than the stereotypical male snoring pattern.
What the science says
The 2025 updated clinical practice guidelines recommend positive airway pressure (PAP) devices and mandibular advancement devices (custom mouthguards) as first-line therapies for mild to moderate obstructive sleep apnea. At-home sleep testing is now widely available, often covered by insurance, and can be done in a single night.
What you can do now
- If your partner has mentioned your snoring or observed breath-holding, take this seriously and consult a sleep medicine specialist -- this is not something to manage with lifestyle tips alone
- Sleeping on your side rather than your back significantly reduces airway collapse. A body pillow or a tennis ball sewn into the back of a sleep shirt are low-tech but effective positional tools
- Alcohol before bed worsens OSA substantially -- it relaxes upper airway muscles, increasing both snoring and apnea events
- Nasal strips can reduce mild snoring caused by nasal congestion but do not address OSA
Problem 4: Early morning waking and poor sleep maintenance
You fall asleep fine but wake at 4 or 5am and can't get back to sleep. This is a distinct pattern from sleep onset insomnia and responds to different interventions.
What's happening
Early morning waking is often associated with elevated cortisol and a dysregulated circadian rhythm. In athletes, it frequently signals accumulated training stress or overreaching -- the nervous system is activating early because it's still in a state of high physiological demand. It can also be a feature of anxiety, depression, or perimenopause.
What the science says
Light therapy is one of the most evidence-backed and underused interventions for circadian rhythm dysregulation. Bright light exposure in the morning -- ideally natural sunlight within 30 minutes of waking -- anchors your circadian rhythm and makes it more consistent night to night. Blue light-blocking amber glasses worn in the evening have shown improvements in sleep onset and quality in athlete research. CBT-I sleep restriction therapy is particularly effective for early morning waking because it consolidates the sleep window and rebuilds sleep pressure that makes resisting early waking easier over time.
What you can do
- Avoid looking at the clock when you wake early -- clock-watching activates the stress response and makes returning to sleep harder. Turn clocks away from the bed
- Get bright light exposure within 30 minutes of your target wake time every morning, including weekends -- this is one of the highest-leverage circadian anchors available and it costs nothing
- If early waking coincides with a heavy training block, treat it as a readiness signal alongside your HRV. Reduce intensity and monitor whether the pattern resolves with load reduction
Problem 5: Pre-competition or pre-event sleep disruption
You sleep well normally. But the night before a race, a big presentation, or any high-stakes event, you can't sleep at all.
What's happening
Pre-competition insomnia is near-universal among athletes. Adrenaline, anticipatory anxiety, and an elevated nervous system override normal sleep pressure. It's not a sleep disorder -- it's a normal physiological response to a perceived high-stakes situation.
What the science actually says -- and this is genuinely reassuring
One night of poor sleep before competition has a smaller impact on performance than athletes believe, particularly for short-duration or high-intensity efforts. The physiological arousal that disrupts sleep actually supports acute performance. Many athletes who report their worst pre-race sleep go on to have their best performances -- the nervous system activation that kept them awake is the same activation that drives output on race day.
What matters more is the night two nights before competition -- that sleep is a stronger predictor of performance than the immediately preceding night. This is where to focus your discipline, not on forcing sleep the night before when adrenaline is working against you.
What you can do
- Protect your sleep two nights before the event as a non-negotiable priority -- this is where the performance dividend is actually paid
- On the night before, reduce the pressure to sleep. Give yourself permission to rest quietly even if you don't fully sleep -- passive rest still provides meaningful recovery benefit
- Use your exact normal pre-sleep routine -- familiarity signals to the nervous system that the situation is manageable
- Avoid any stimulants after noon in the 48 hours before competition
Problem 6: Travel and time zone disruption
If your training involves early morning sessions, frequent travel, or regularly crossing time zones, your circadian rhythm is absorbing disruption that compounds directly with training stress.
What's happening
Your circadian rhythm governs the timing of sleep stages, hormone release, and core temperature -- all of which affect training performance and recovery. Crossing time zones shifts this rhythm out of sync with local time. Even without crossing time zones, consistent early morning alarms that cut into REM-rich final sleep hours create a chronic REM deficit that accumulates over weeks.
What the science says
Melatonin is one of the most evidence-supported supplements specifically for circadian rhythm disruption -- not as a sedative, but as a time-giver that helps reset the biological clock. Small doses (0.5 to 1 mg) taken at the target bedtime at the destination are more effective for jet lag than the large doses (5 to 10 mg) commonly sold in pharmacies. Morning light exposure at the destination is the strongest available reset signal and it costs nothing.
One often-missed travel tip: for the first 48 hours after crossing multiple time zones, schedule your hardest training sessions at the time of day that corresponds to your body's normal peak output at home -- not at local time. Your neuromuscular performance and injury resistance haven't adjusted yet, and training at the wrong biological time increases both perceived effort and injury risk.
What you can do
- Begin shifting your sleep and wake time 2 to 3 days before eastward travel (the harder direction) by going to bed and rising 30 to 60 minutes earlier each day
- Use 0.5 to 1 mg melatonin at target destination bedtime for the first 3 to 4 nights after crossing 3 or more time zones
- Get outside in morning light at your destination immediately -- it's the fastest reset available
- For chronic early morning training sessions: protect the final 60 to 90 minutes of your sleep window wherever possible -- that's where REM lives and where the cognitive and motor recovery happens
The supplements with actual evidence
Most sleep supplements are oversold. These four have genuine clinical support worth knowing about -- starting with the cheapest options first.
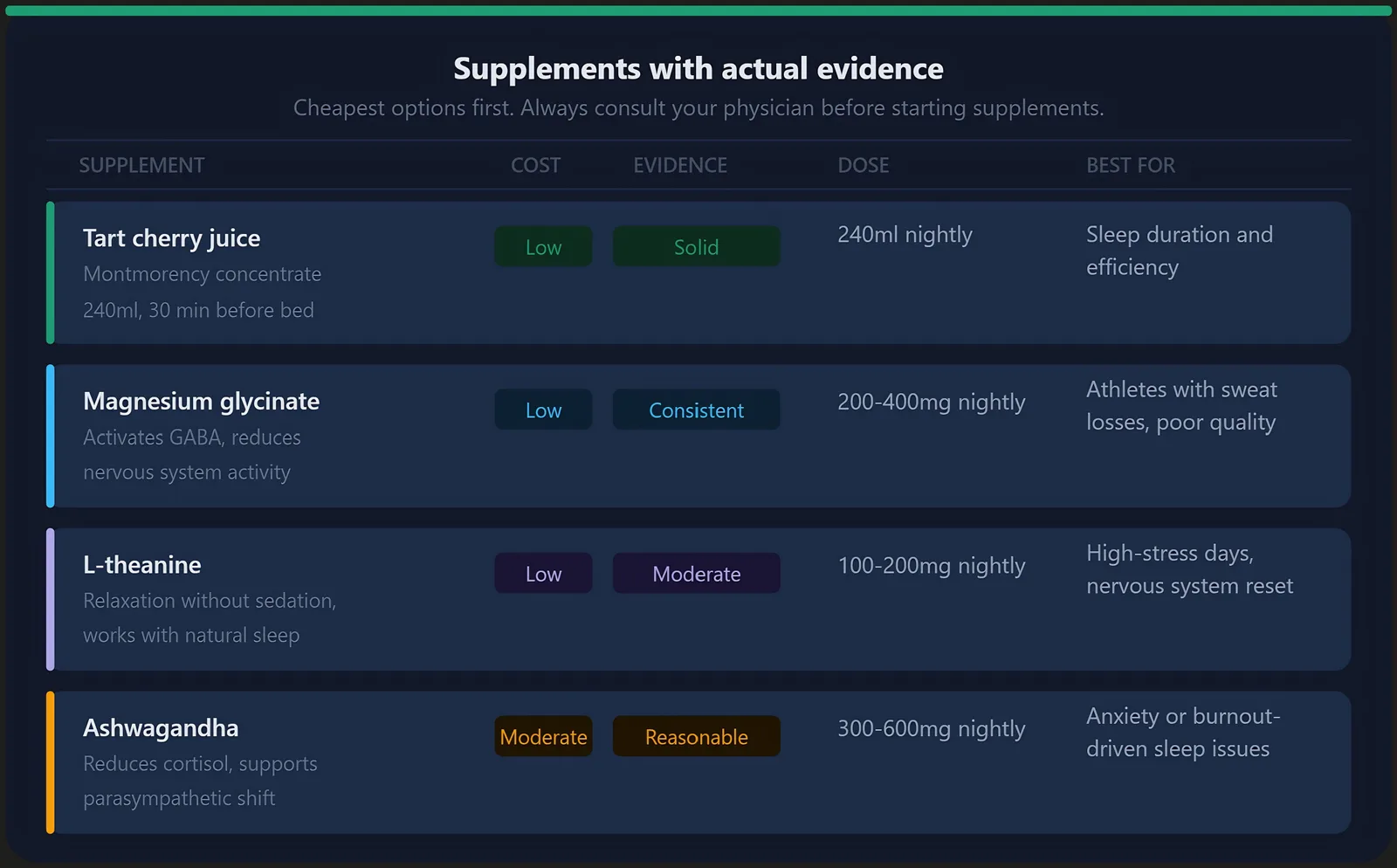
Tart cherry juice Tart cherries contain natural melatonin and anthocyanins that improve sleep quality. A pilot study of people with insomnia found that drinking tart cherry juice increased total sleep time by 84 minutes as measured by polysomnography -- striking numbers for a food-based intervention. The juice used in research is concentrated Montmorency tart cherry juice, not the sweetened blends in most grocery stores. 240ml taken 30 minutes before bed is the studied dose.
Magnesium glycinate Magnesium plays a role in GABA activation -- the primary inhibitory neurotransmitter that quiets the nervous system for sleep. Many athletes are mildly deficient due to sweat losses. Magnesium glycinate is among the best-tolerated forms. 200 to 400 mg taken 30 to 60 minutes before bed is the commonly used dose.
L-theanine An amino acid found in green tea that promotes relaxation without forcing sleep. It works with the natural sleep process rather than overriding it. 100 to 200 mg taken 30 to 60 minutes before bed is the commonly studied dose. Particularly useful on high-stress days when the nervous system needs help downregulating.
Ashwagandha An adaptogen that works by reducing cortisol and supporting the parasympathetic shift needed for sleep onset. Most effective when sleep problems are driven by anxiety or high training load. Less useful for circadian or structural issues.
What to skip High-dose melatonin (5 to 10 mg) is routinely oversold for general insomnia -- low-dose timing-targeted use is more appropriate. Prescription sleep aids suppress REM and deep sleep architecture, making them counterproductive for athletes except in specific short-term clinical situations discussed with a physician.
Strategic napping: when it helps and when it doesn't
Napping has solid scientific support as a recovery tool -- with an important caveat that depends entirely on whether your nighttime sleep is already working.
If you sleep well at night
A well-timed nap is a legitimate performance tool. Research published in 2025 and 2026 across multiple systematic reviews found that daytime naps improve alertness, reaction time, sprint performance, perceived recovery, and cognitive function in athletes -- even those who got adequate sleep the night before.
The rules that the research supports:
- Keep it under 30 minutes for a quick alertness reset -- this avoids entering deep sleep and the grogginess (sleep inertia) that follows waking from it
- A 90-minute nap allows a full sleep cycle including deep sleep, producing more profound recovery -- but only use this when you have significant sleep debt and enough time to fully wake before training or competition
- Nap between 1pm and 4pm -- this aligns with the natural post-lunch dip in alertness and minimizes disruption to your nighttime sleep onset
- Allow at least 30 minutes between waking from a nap and any hard training session to let alertness fully return
If you struggle with nighttime sleep
Proceed with real caution here. Napping reduces sleep pressure -- the biological drive that builds throughout the day and makes falling asleep at night possible. A nap that feels helpful in the moment can make the underlying nighttime problem measurably worse by stealing the pressure your body needs to initiate and maintain sleep later.
If you're working through CBT-I -- either self-directed or with a therapist -- the protocol typically recommends avoiding naps entirely during the active treatment phase for exactly this reason. Once your nighttime sleep has stabilized, strategic short naps can be reintroduced carefully.
The one exception: if you had a genuinely terrible night (under 5 hours) and have hard training scheduled, a short 20-minute nap before 1pm is a reasonable bridge -- prioritizing the session quality over the strict no-nap rule. Keep it short, keep it early, and monitor how it affects the following night.
When nothing is working: the escalation path
If you've tried consistent sleep hygiene, addressed the obvious culprits like alcohol and caffeine timing, and still can't sleep reliably -- you're not failing at something simple. You may have a structural problem that self-help can't reach. Here's the honest escalation path, free options first.
Step 1 -- Try free CBT-I resources
Most people who attempt CBT-I do so inconsistently through a single tip they read online. A full structured program is different -- and several free ones exist.
The best free starting point is the CBT-i Coach app, developed by the US Department of Veterans Affairs in partnership with Stanford University. It's free on iOS and Android, evidence-based, and includes a structured sleep diary, psychoeducation, and guided implementation of core CBT-I techniques. It is not a tracking app -- it actively walks you through the behavioral change protocol.
Insomnia Coach (also from the VA) offers a structured five-week standalone program for anyone struggling with chronic sleep issues. Also completely free on iOS and Android.
YouTube has a growing library of legitimate CBT-I walkthroughs from clinicians and sleep medicine departments. Search specifically for "CBT-I sleep restriction" and "stimulus control insomnia" to find protocol-based content rather than generic sleep hygiene advice. The University of Michigan and Stanford sleep medicine departments have both published free video resources worth finding.
One important note: CBT-I is uncomfortable at first because sleep restriction temporarily increases sleepiness before it improves sleep consolidation. Most people quit during that window. Staying with it consistently for two to three weeks is where the results happen.
Step 2 -- Rule out sleep apnea
If self-directed CBT-I hasn't moved the needle after four weeks of consistent effort, the single most important next step is ruling out obstructive sleep apnea. It renders every other intervention less effective because sleep architecture is being physically disrupted dozens of times per night regardless of what you take or do. At-home sleep testing is widely available, often covered by insurance, and takes a single night. If OSA is present and treated, many people find their other sleep problems resolve substantially on their own.
Step 3 -- Address the hormonal layer if relevant
For perimenopausal and menopausal women whose primary driver is night sweats and hot flushes that lifestyle interventions haven't resolved, HRT with a NAMS-certified menopause specialist is the evidence-based next step. The research on HRT and sleep is strong. The conversation around risks has shifted significantly -- the benefits for most healthy women in early menopause are substantial and the risks lower than previously communicated. A NAMS-certified specialist rather than a general practitioner is worth seeking out, as the literature has moved faster than general practice in this area.
Step 4 -- Formal CBT-I with a therapist
If self-directed CBT-I hasn't been sufficient, working with a certified CBT-I therapist -- in person or via telehealth -- is the clinical gold standard for persistent insomnia. The structured protocol typically runs 6 to 8 sessions. Some insurance plans cover it. The Society of Behavioral Sleep Medicine at behavioralsleep.org maintains a searchable directory of certified providers.
Step 5 -- A comprehensive sleep study
If the above haven't resolved the issue, a full in-lab polysomnography (PSG) can identify sleep architecture problems, movement disorders like restless leg syndrome or periodic limb movement disorder, and other structural issues that at-home testing misses entirely. This is the clinical gold standard and where sleep medicine earns its name.
Step 6 -- Short-term pharmacological support as a bridge
For some people, a short course of medication can break a chronic insomnia cycle that has become self-perpetuating. Newer dual orexin receptor antagonists like suvorexant or lemborexant have a better profile for athletes than older benzodiazepines or z-drugs because they don't suppress deep sleep architecture as significantly. This is a bridge strategy, not a solution -- most effective when combined with concurrent CBT-I so behavioral change is happening during the window when sleep is pharmacologically supported. Discuss this with your physician.
One more thing: are you anxious about your sleep score?
There's a clinical term for it -- orthosomnia -- and it's increasingly common among wearable users. The anxiety about getting a good sleep score can itself become a cause of poor sleep, creating a loop where the data meant to help you starts working against you.
If you find yourself lying awake worrying about what your tracker will show, or changing your behavior based on a single night's reading rather than a trend, that's worth noticing. Your sleep score is a directional signal over time -- not a nightly grade. A single poor reading tells you almost nothing. A trend over 7 to 10 days tells you something real.
Use the data as a tool, not a verdict.
What your Fit PA data tells you about your sleep
Your sleep score, HRV trend, and Readiness Score together tell a daily story about the quality of your recovery window. When sleep is genuinely good, HRV stabilizes or rises. When sleep is disrupted -- regardless of the reason -- HRV drops and readiness follows.
Use that connection in both directions. A persistently low readiness score is often a sleep problem wearing a training costume. And improving your sleep -- through any of the interventions above that match your specific situation -- is one of the fastest routes to a meaningful improvement in your training data without changing a single session.
Sleep disorders are medical conditions, not character flaws or training problems. Treating them is performance optimization by another name.
Check your sleep trend and Readiness Score in your Fit PA dashboard. If the pattern isn't moving in the right direction, this article is your starting point.